
Paul Pharoah is Professor of Cancer Epidemiology at the University of Cambridge, where he leads research on the molecular pathology of breast and ovarian cancer and genetic susceptibility to the common cancers (primarily breast, ovarian and colorectal). This interview is based around a commentary in Cancer Cell, which you can read here.
Critics of cancer screening often say that “screening has never been shown to save lives”, whereas lots of studies of cancer screening report that they do save lives. What is going on? Is this a case of semantics or are there real differences in interpretation?
It’s both semantics and interpretation. Lots of randomized controlled screening trials have cancer-specific mortality as the endpoint of interest. Trials for some cancers reasonably convincingly show a reduction in the mortality from the cancer of interest- be that lung, colorectal, or otherwise. The question, then, is “Is there a nominally statistically significant reduction in all-cause mortality?”. When ‘screening protagonists’ say it saves lives, it’s not always clear whether they mean all-cause mortality or cause-specific mortality. For the critics, when they say screening has never been shown to save lives, what they mean is all-cause mortality. When critics say that, what they mean is there isn’t a nominally statistically significant reduction in all-cause mortality- the p-value isn’t <0.05, and therefore there isn’t a reduction in all-cause mortality. I think that’s flawed statistical inference; there may be a reduction in all-cause mortality that just isn’t statistically significant, and one of the big problems is that the reduction in all-cause mortality that you might expect may actually be quite small. If you’re screening for colorectal cancer and you reduce the deaths from colorectal cancer, the expected reduction in all-cause mortality will be small- even huge trials won’t detect it. If you see a reduction of any sort- which isn’t nominally statistically significant- you may still regard that as evidence of saving lives. It’s a bit of a complex between semantics, exact definitions and misinterpretation of data that results in these completely diverging opinions.
The analysis of all-cause mortality in cancer screening trials in your comment article is new, can you explain what you have done?
There are quite a few randomized control cancer screening trials that have been published. We don’t have any new data; we’ve looked at data that has already been published and put it together and interpreted it in a different way. There have been lots of studies where people have pooled data from cancer screening trials for specific cancers and published those results. We looked across all the trials we knew about and pooled the findings. We then took an estimate from the pool results of the cancer-specific mortality reduction and asked the question: “If this is the reduction of cancer-specific mortality, what would we expect the reduction in all-cause mortality to be?”. We compared what you would expect in those trials- which we show in figure 1.
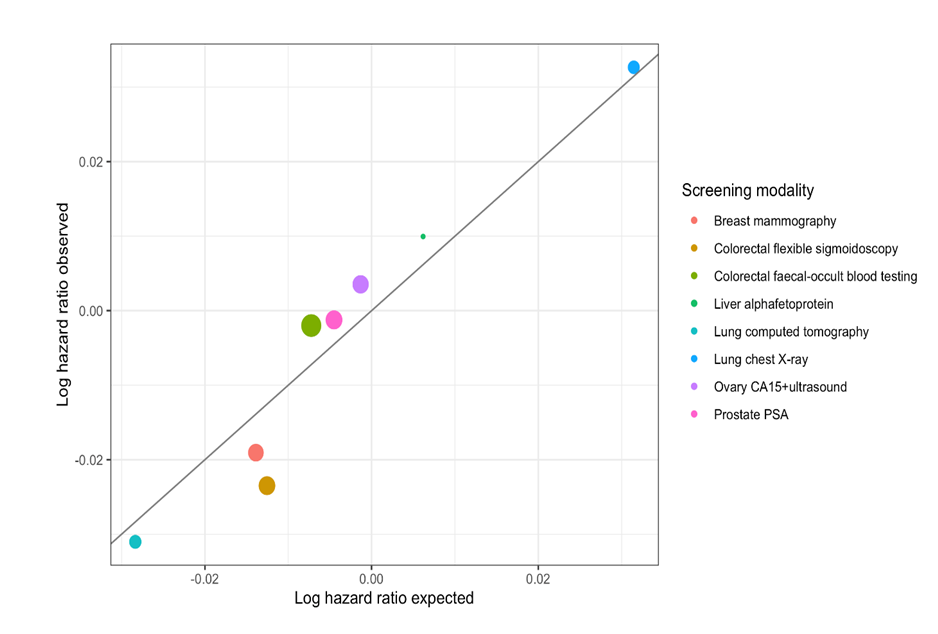
If you plot the observed reduction in all-cause mortality against the expected, there’s quite a strong association. Even if the all-cause mortality is not particularly significant in a nominal sense, that doesn’t mean it isn’t real. People often use this dichotomy of- is it statistically significant, there isn’t an effect, so if it’s not significant there isn’t an effect, and there’s a lot of discussion in the statistical world at the moment to decide if it’s appropriate to say there’s no effect just because the p values is less than 0.05. What might be more appropriate is to use a Bayesian approach, to say how likely it is that the all-cause mortality reduction is small, and for several cancers, you can say there’s a reasonably high chance that there is a small but real reduction in all-cause mortality, even if the p-value isn’t 0.05 or less.
Is it true that even using the yardstick of sceptics, you have now shown that both breast screening and bowel cancer screening saves lives?
If we want to show that all-cause mortality is significantly reduced with a nominal value of p <0.05, then the effect of bowel cancer screening on all-cause mortality is statistically significant. Even the sceptics can’t really claim there’s no significant reduction in all-cause mortality. For breast cancer screening, our estimate of the all-cause mortality reduction is still not quite statistically significant, so sceptics using the yardstick of p <0.05 would still maintain that there’s no reduction or lives saved. What we’ve done is take a more nuanced approach to see how likely it is using a Bayesian approach- when you do that, it’s quite likely that there’s a reduction in all-cause mortality from breast screening.
What is the significance of the plot of the observed versus expected hazard ratios?
The black line is observed equals expected, and the point is that mostly, the observed is close to the expected. We’re trying to show that what is observed in these trials, the all-cause mortality reduction, is very close to what we’d expect given the magnitude of the reduction in cause-specific mortality. For colorectal cancer, for flexible sigmoidoscopy, the tan circle (in figure 1) represents the effect size on all-cause mortality. Colorectal cancer only accounts for a very small proportion of all mortality, so even if you have an effective screening tool that has a big effect on colorectal cancer mortality, you’re still only going to have a small effect on all-cause mortality and what we’ve shown here is that there is an effect on all-cause mortality that’s pretty much in-line with what you think it would be in regards to cause-specific mortality.
You represent quite a disparate group of authors: a molecular biologist, a biostatistician, a clinical epidemiologist and a physician-scientist, have you enjoyed working on this paper?
This is something I’ve been thinking about for some time. It was extremely useful to discuss these ideas both with someone with the same background as me- Peter Sasieni, but also to float those ideas to people without those backgrounds to try and explain them and see if it made sense to them. I think that helped to consolidate my ideas and the way I think about the commentary, just by talking to non-experts in that area. I think some of the issues around the underlying biology were of interest, and it was good to go through these things and think about the issues from a different perspective. This project was about consolidating my views from the perspective of other people, and it’s produced an interesting article.
The views expressed are those of the author. Posting of the blog does not signify that the Cancer Prevention Group endorse those views or opinions.
![]()